Introduction
Pain is often spoken about as though it were a single condition, but it isn't.
A sprained ankle, rheumatoid arthritis, diabetic nerve pain and fibromyalgia may all hurt, but they arise from entirely different biological processes.¹⁶ Yet many conversations about medical cannabis ask a single question:
"Does cannabis work for pain?"
From a scientific perspective, that's a little like asking whether antibiotics work for illness. The answer depends entirely on "what is causing the problem in the first place."¹⁶
Researchers increasingly recognise that cannabinoids may interact differently with different pain mechanisms. Understanding those mechanisms may help explain why some patients experience meaningful improvements while others notice only modest or no benefit.¹³
Pain Is an Alarm System, Not a Disease
Pain is one of the body's most sophisticated protective mechanisms. Its primary purpose is to alert us to actual or potential tissue damage. Once the underlying cause has been resolved, the alarm normally quietens.¹⁶
However, pain does not always follow this simple pattern. Depending on where the problem originates, entirely different biological pathways become involved.¹⁶
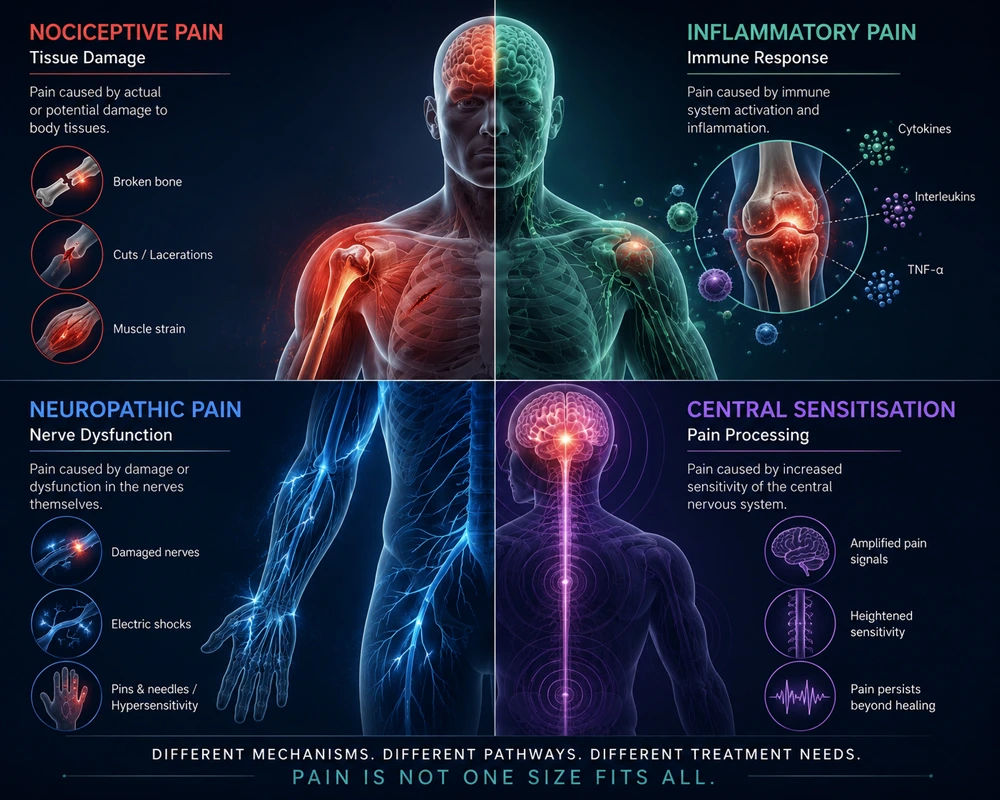
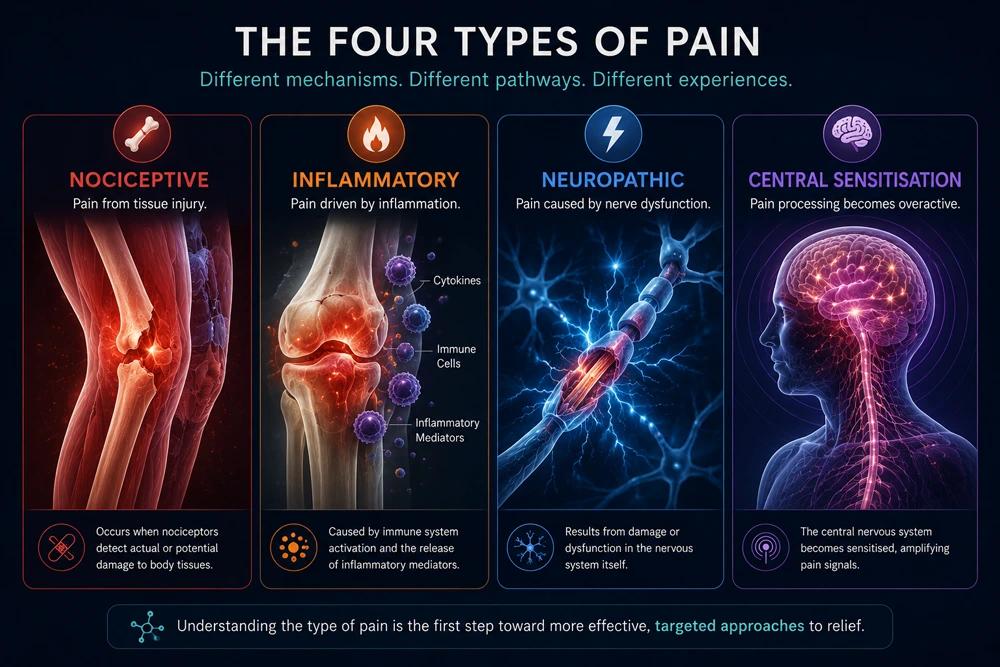
Current pain science generally classifies pain into several broad categories.¹⁶
Nociceptive Pain
This is the pain most people are familiar with. Specialised sensory receptors, called nociceptors, detect tissue injury and send warning signals to the brain.¹⁶
Examples include:
- fractures
- surgical recovery
- burns
- muscle strains
- acute injuries
For many people, nociceptive pain resolves as healing occurs.¹⁶
Inflammatory Pain
Sometimes the pain comes less from the injury itself and more from the body's immune response. Inflammatory cells release chemical messengers, including cytokines, prostaglandins and chemokines, that sensitise nearby nerves, making ordinary movement increasingly painful.¹⁶
Examples include:
- rheumatoid arthritis
- inflammatory bowel disease
- autoimmune disorders
- tendon inflammation
Inflammation is an essential part of healing, but when it becomes persistent, pain may continue long after its protective role has ended.¹⁶
Neuropathic Pain
Neuropathic pain originates within the nervous system itself. Instead of accurately transmitting information, damaged nerves begin generating abnormal electrical signals.¹⁶
Patients often describe:
- burning sensations
- electric shocks
- pins and needles
- hypersensitivity to touch
Common causes include:
- diabetic neuropathy
- multiple sclerosis
- post-herpetic neuralgia
- spinal cord injury
- chemotherapy-induced neuropathy
Neuropathic pain has consistently emerged as one of the pain categories where cannabis-based medicines have shown the most encouraging evidence, although responses remain highly individual.¹²³
Central Sensitisation
Perhaps the most complex category is central sensitisation. Here, the nervous system itself becomes increasingly sensitive over time. Pain processing pathways within the brain and spinal cord amplify incoming signals, causing ordinary sensations to become painful and painful sensations to feel even more intense.¹⁶
Conditions associated with central sensitisation include:
- fibromyalgia
- chronic fatigue syndrome
- persistent post-surgical pain
- some chronic headache disorders
Researchers continue to investigate how changes within the Endocannabinoid System may contribute to this heightened pain sensitivity.³⁵
So Where Does Cannabis Fit?
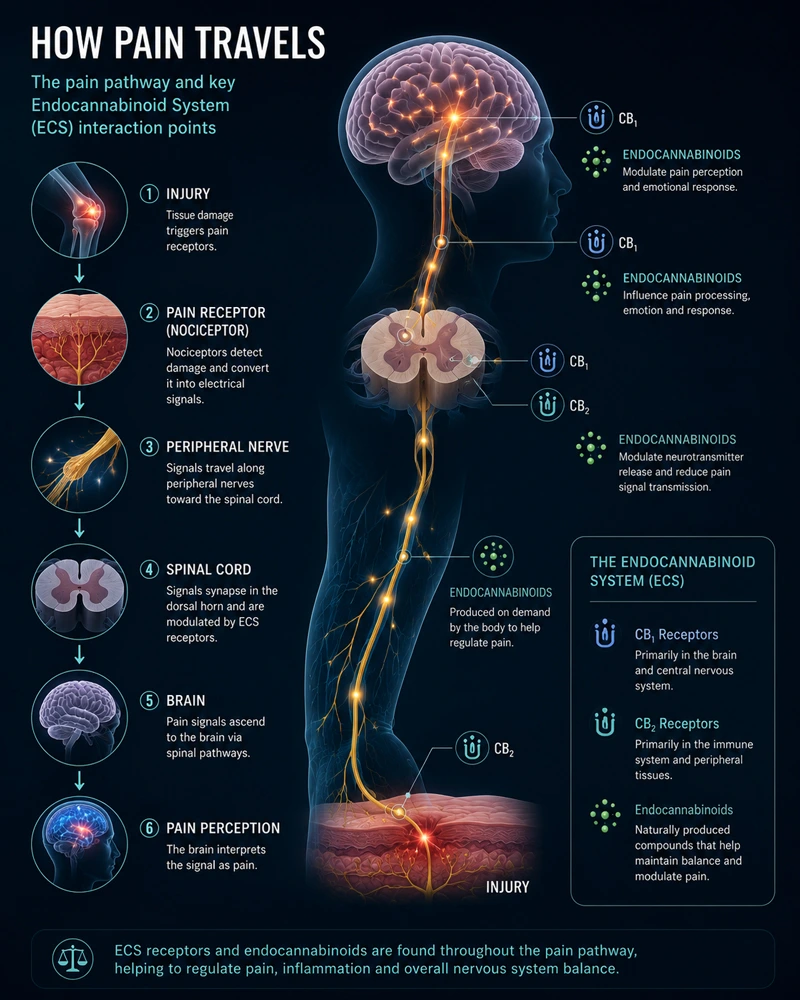
The Endocannabinoid System (ECS) plays an important role in regulating pain signalling throughout the brain, spinal cord, immune system and peripheral tissues.³
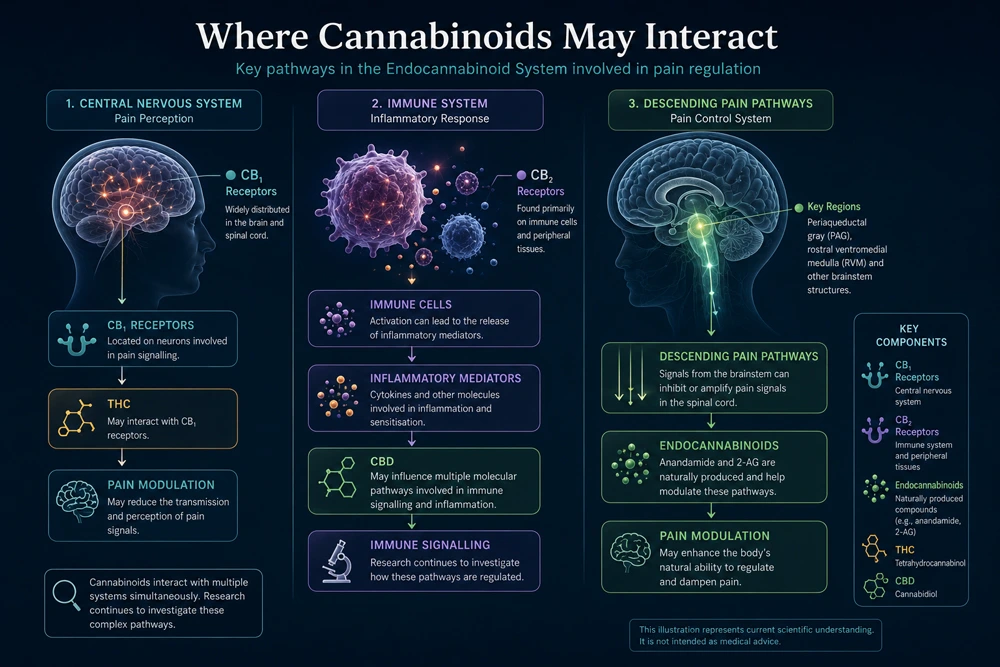
Rather than functioning as a conventional painkiller, cannabinoids appear to influence several biological pathways involved in pain processing.³⁴
Different cannabinoids may affect different components of these pathways.³⁴
Neuropathic Pain
In neuropathic pain, THC has been studied for its interaction with CB₁ receptors within the central nervous system.³
Activation of these receptors may alter the transmission and perception of pain signals, potentially reducing the intensity of neuropathic pain in some patients.¹³
Inflammatory Pain
Inflammatory pain involves complex interactions between immune cells and inflammatory mediators.
Cannabidiol (CBD) does not act through a single receptor. Instead, laboratory and clinical research suggests it may influence inflammatory signalling through multiple pathways, including cytokine regulation, transient receptor potential (TRP) channels, serotonin receptors and the preservation of endogenous cannabinoids such as anandamide.³⁴
These mechanisms remain areas of active investigation.³⁴
Central Sensitisation
Researchers are also exploring how cannabinoids influence the brain's descending pain modulation system. A network responsible for amplifying or suppressing incoming pain signals.³
Although this field is still developing, modulation of these pathways may partly explain why some patients with fibromyalgia or persistent pain syndromes report improvements in pain perception, sleep quality and overall wellbeing.²³⁵
The important point is this:
Cannabis is unlikely to work through one universal mechanism because pain itself does not arise from one universal mechanism.¹³¹⁶
Why Do Studies Reach Different Conclusions?
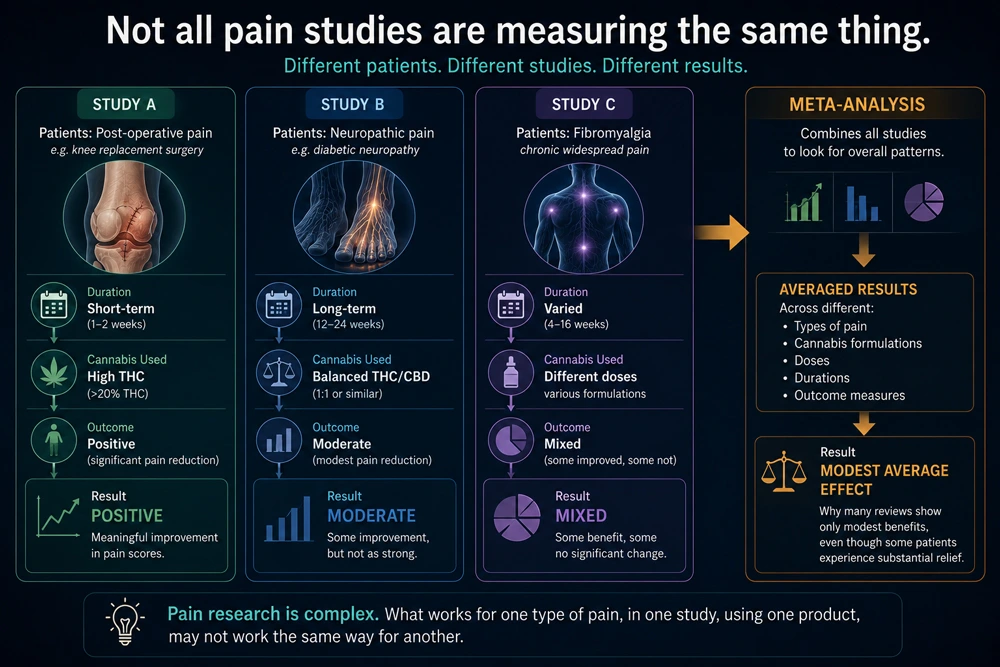
News headlines often appear contradictory. One study reports cannabis significantly reduces pain, and another concludes the benefits are modest. Neither is necessarily wrong.
Pain research is extraordinarily difficult because researchers are often studying entirely different patient populations.¹²
Someone recovering from knee replacement surgery is biologically very different from someone living with twenty years of diabetic neuropathy.¹²
The studies themselves also vary considerably.
Researchers may investigate:
- different pain conditions
- different cannabis formulations
- varying THC:CBD ratios
- different doses
- treatment durations ranging from days to months
- inhaled, oral or sublingual administration
- patient-reported outcomes versus objective clinical measures
These differences make direct comparison challenging and help explain why systematic reviews often conclude that overall benefits are modest, while individual patients may experience substantial improvements.¹²
This variability is precisely why modern cannabinoid research is shifting away from asking whether cannabis works and towards understanding "who may benefit, under what circumstances and why."¹²
The Future Is Precision Cannabinoid Medicine
Medicine is increasingly moving away from one-size-fits-all treatment.⁴ Cannabinoid science appears to be following the same path.³⁴
Current areas of investigation include:
- individual cannabinoid profiles
- terpene composition
- flavonoid interactions
- genetic variation in cannabinoid receptors
- Endocannabinoid System biomarkers
- personalised dosing strategies³⁴
Rather than searching for a single cannabinoid capable of treating every patient, researchers are exploring how combinations of cannabinoids and other cannabis-derived compounds may be matched to specific biological mechanisms underlying different pain conditions.³⁴
While many questions remain unanswered, advances in molecular biology, pharmacology and precision medicine are rapidly expanding our understanding of how cannabis-based medicines may eventually become more personalised.³⁴

Conclusion
Pain is not a single disease, and it is unlikely that one cannabinoid, or one cannabis product, will benefit every person in the same way.¹³
As our understanding of the Endocannabinoid System continues to evolve, researchers are moving beyond the simple question of whether cannabis works for pain.³
Instead, they are asking a more important question: "Which cannabinoid profile works best for which type of pain?"
The answer to that question may shape the future of cannabinoid medicine and lead to more precise, evidence-informed approaches to pain management.³⁴
References
- Wang L, Hong PJ, May C, et al. Medical Cannabis or Cannabinoids for Chronic Pain: A Systematic Review and Meta-analysis. BMJ. 2021;374.
- Häuser W, Petzke F, Fitzcharles MA. Efficacy, tolerability and safety of cannabis-based medicines for chronic pain management. Drugs. 2018;78(17):1757–1765.
- Finn DP, Haroutounian S, Hohmann AG, et al. Cannabinoids, the Endocannabinoid System and Pain. Pain. 2021;162(Suppl 1)–S25.
- Ibeas Bih C, Chen T, Nunn AVW, Bazelot M, Dallas M, Whalley BJ. Molecular Targets of Cannabidiol in Neurological Disorders. Neurotherapeutics. 2015;12:699–730.
- MacCallum CA, Russo EB. Practical Considerations in Medical Cannabis Administration and Dosing. European Journal of Internal Medicine. 2018;49:12–19.
- International Association for the Study of Pain (IASP). IASP Terminology and Classification of Pain.
Disclaimer: This blog supports responsible cannabis use. The information contained in this article is for educational and informational purposes only and is not intended as health or medical advice. Always consult a physician or other qualified health provider regarding any questions you may have about a medical condition or health objectives.